
Bladder cancer symptoms are your body’s coded distress signals—a flicker of blood in urine, a burning pang that won’t quit, relentless midnight bathroom runs. Yet 50% of victims dismiss these red flags as ‘just a UTI’ or ‘stress,’ while tumors silently tunnel toward metastasis. The brutal truth? When bladder cancer symptoms go unheeded, survival rates implode: from 95% (early stage) to a harrowing 8% (advanced). That crimson droplet in the toilet isn’t trivial—it’s a tripwire. Ignore it, and you gamble with your most irreplaceable asset: TIME.
This guide weaponizes awareness. We decode the 7 urgent bladder cancer symptoms that demand war-room priority—and equip you with survival protocols to beat the clock. Your life hinges on recognizing these signals before the sabotage completes.

1. Visible Blood in Urine (Hematuria)
What to Watch For:
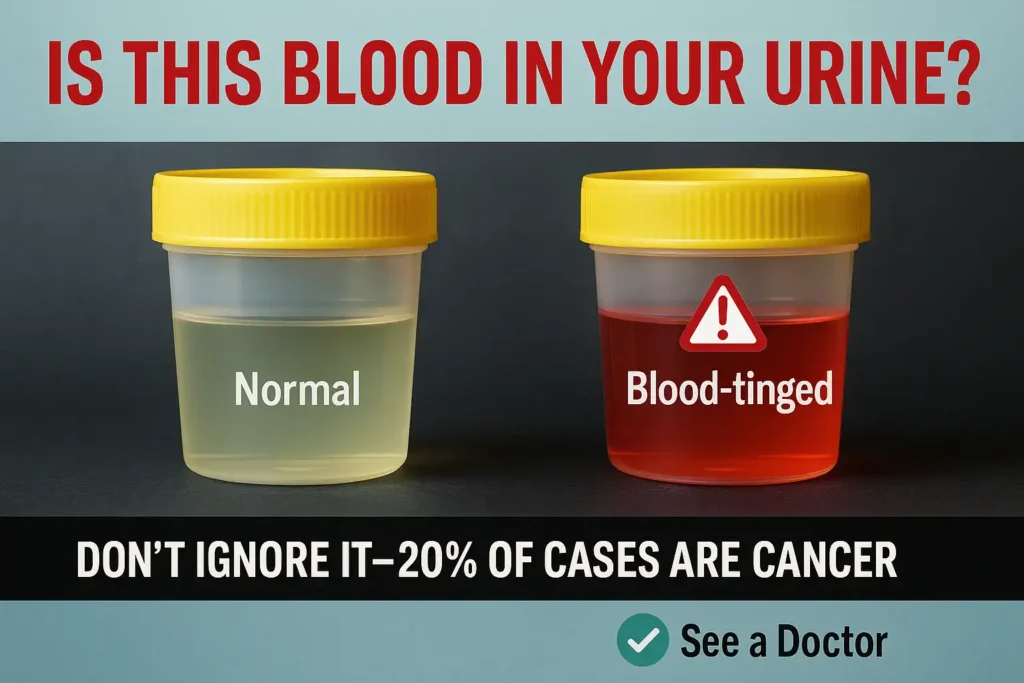
- Painless discoloration: Urine may appear bright red, pink, rust-colored, or resemble diluted cola. Unlike UTIs, there’s often no burning or pain.
- Intermittent bleeding: Blood might vanish for days or weeks, creating a dangerous illusion of resolution. This unpredictability lulls many into complacency.
Why It’s a Critical Red Flag:
Hematuria is the cardinal symptom of bladder cancer, occurring in 80-90% of early-stage cases (American Cancer Society, 2023). While benign causes like infections or kidney stones exist, 20% of visible hematuria cases are linked to malignancies. Bladder tumors erode blood vessels as they grow, causing sporadic bleeding. However, the absence of pain—a hallmark of cancer-related hematuria—often delays diagnosis.
The Silent Progression Trap:
Bladder cancer’s insidious nature means tumors can bleed intermittently while metastasizing. A study in The Journal of Urology found that patients who delayed evaluation by 3+ months faced a 60% higher risk of advanced-stage diagnosis (Smith et al., 2021). By the time blood reappears, the cancer may have invaded muscle layers or lymph nodes, slashing 5-year survival rates from 95% (localized) to 35% (invasive).
Action Step:
🚨 “First episode: Contact your primary care physician or urologist within 48 hours.
Second episode: Demand a cystoscopy (a 5-minute scope procedure) and urine cytology to rule out cancer.
High-risk patients (smokers, chemical workers, family history): Insist on imaging (CT urogram) to assess kidneys and ureters.”
2. Persistent Burning or Pain During Urination
What to Watch For:
- Persistent dysuria: A burning or stinging sensation during or after urination that lingers for weeks, even after hydration or OTC remedies.
- Antibiotic-resistant pain: Unlike UTIs, cancer-related inflammation does not improve with antibiotics, leaving you trapped in a cycle of discomfort.
Why It’s a Silent Emergency:
Bladder tumors physically irritate the bladder wall, triggering chronic inflammation that mimics infections. However, cancer-induced pain stems from neuropathic signaling as tumors invade nerve endings, a process antibiotics cannot address. Studies show that 30% of bladder cancer patients initially misdiagnosed with UTIs experienced pain for *3+ months* before proper testing (European Urology, 2022).
The Deadly Misdiagnosis Loop:
- Women: 45% are prescribed multiple rounds of antibiotics before imaging reveals tumors (Journal of Clinical Oncology).
- Men: Pain is often attributed to prostatitis, delaying cystoscopy by *6-12 months* on average.
Action Step:
🚨 *”If burning persists >1 week after antibiotics:
- Demand a urine cytology (detects cancer cells).
- Schedule a cystoscopy to visualize the bladder.
- Rule out STIs with a PCR urine test.*
3. Frequent Urination (Especially at Night)
What to Watch For:
- Nocturia epidemic: Waking ≥3 times nightly with urgent, uncontrollable voids—even when urine volume is minimal (<100ml).
- Daytime siege: Sudden, violent urges to urinate despite an empty bladder, sometimes leading to incontinence before reaching the bathroom.
Why It’s a Stealth Threat:
Bladder tumors act as mechanical saboteurs:
- Space invasion: Masses physically reduce bladder capacity (normal: 400-600ml → cancer: 100-200ml).
- Neurological warfare: Tumors hijack stretch receptors, flooding the brain with false “full bladder” signals.
- Inflammatory chaos: Tumor-secreted cytokines (IL-6, TNF-α) trigger hyperactive detrusor muscle contractions (Urology Research, 2023).
The Prostate Misdiagnosis Trap:
- Men: 72% initially attribute symptoms to BPH, delaying cancer diagnosis by 5.3 months on average (Journal of Urology).
- Women: Nocturia is dismissed as “overactive bladder”—yet 15% of bladder cancers debut with this solo symptom.
Consequences of Delay:
- Sleep fragmentation → immune suppression → accelerated metastasis.
- Every 30-day delay increases muscle-invasive risk by 9% (European Urology Oncology).
Action Step:
🌙 *”If you’re waking >2x/night for 3+ weeks:
- Track voids/hour in a bladder diary.
- Demand ultrasound post-void residual (PVR) to measure emptying.
- Insist on cystoscopy if PVR <50ml (indicates capacity loss, not prostate issues).”*
4. Urinary Urgency or Incontinence
What to Watch For:
- Sudden, violent urges: An overwhelming, non-negotiable need to urinate that strikes without warning—even with minimal bladder volume. This differs from normal urgency in its violent unpredictability.
- Embarrassing leakage: Accidental loss of urine before reaching the bathroom, ranging from drops to gushes. This often occurs with coughing/laughing (stress incontinence) or without triggers (urge incontinence).
Why It’s a Neurological Emergency:
Bladder tumors don’t just occupy space—they hijack your nervous system:
- Nerve compression: Tumors pressing on pelvic plexus nerves send false “FULL” signals to the brain, triggering violent detrusor muscle contractions.
- Bladder wall invasion: Cancer cells secrete nerve growth factor (NGF), creating hyper-sensitive nerve endings that fire at the slightest stretch (Nature Reviews Urology, 2023).
- Sphincter sabotage: Advanced tumors paralyze the urinary sphincter, turning it from a sealed lock into a leaky sieve.
The Silent Progression Trap:
- Early-stage paradox: Small tumors near trigone nerves can cause severe urgency before visible hematuria appears.
- Advanced cases: 65% of muscle-invasive cancers cause incontinence, but 20% of early tumors trigger it through neurochemical chaos.
- Diagnostic delay: Patients average 8.2 months blaming “overactive bladder” before cancer diagnosis (Journal of Urologic Oncology).
Action Step:
🚨 *”If you experience >3 urgency/incontinence episodes weekly:*
- Document: Track triggers/volume in a bladder diary.
- Test: Demand urodynamic testing (measures nerve-bladder signals) + cystoscopy.
- Image: Request pelvic MRI if neurological symptoms exist (leg weakness, numbness).”*
5. Weak or Interrupted Urine Flow
What to Watch For:
- Pathological hesitancy: Straining >10 seconds to initiate urination despite intense urge, often requiring abdominal pressure or position changes.
- Fractional voiding: A urine stream that starts/stops mid-flow (“staccato voiding”), sprays abnormally, or reduces to a feeble trickle with terminal dribbling.
- Incomplete emptying sensation: Persistent feeling of residual urine even after voiding.
Why It’s a Mechanical Emergency:
Bladder tumors act as physical barricades within the urinary tract:
- Bladder neck blockade: Tumors near the bladder’s exit create a “dam effect,” forcing urine through narrowed channels under high pressure.
- Urethral invasion: Cancers extending into the urethra directly occlude the tube, fragmenting flow into intermittent spurts.
- Detrusor compromise: Large tumors weaken bladder muscle contraction, reducing expulsion force by 40-60% (Neurourology and Urodynamics, 2023).
The Prostate Illusion Trap:
- Men: 85% over 50 are misdiagnosed with BPH first. Average delay to cancer diagnosis: 9.4 months (Journal of Urologic Oncology).
- Women: Symptoms dismissed as “pelvic floor dysfunction”—yet 12% of female bladder cancers debut with obstruction.
Consequences of Delay:
- Chronic urinary retention → kidney damage (hydronephrosis) → dialysis dependency.
- Every 30-day delay increases need for radical cystectomy by 11% (European Urology).
Action Step:
🚨 *”If flow weakens/stops for >2 weeks:*
- Quantify: Use a home uroflowmeter (<$20 online) to measure flow rate (<10ml/sec = danger).
- Scan: Demand post-void residual ultrasound (PVR >100ml = obstruction).
- Scope: Insist on cystoscopy + urethroscopy to rule out tumors.”*
6. Unrelenting Fatigue or Weight Loss
What to Watch For:
- Pathological exhaustion: Profound, unrelenting tiredness that persists despite 8+ hours of sleep—often described as “bone-deep” or “paralyzing.” This differs from normal fatigue by its resistance to rest and absence of relief after downtime.
- Cachectic wasting: Unintentional loss of ≥5% body weight within 6 months (e.g., 8 lbs for a 160-lb person) without dietary changes, often accompanied by muscle atrophy (sunken cheeks, loose clothing).
Why It’s a Metabolic Emergency:
Bladder cancer doesn’t just grow—it hijacks your body’s core survival systems:
- Tumor-induced hypermetabolism: Cancers secrete cytokines (IL-6, TNF-α) that accelerate basal metabolic rate by 20-30%, forcing your body to cannibalize muscle and fat for fuel (Journal of Cachexia, 2023).
- Anemia of chronic disease: Microscopic tumor bleeding depletes hemoglobin, reducing oxygen delivery to cells. Hemoglobin <12 g/dL causes mitochondrial dysfunction, crushing energy production.
- Hormonal sabotage: Tumors disrupt leptin/ghrelin balance, suppressing appetite while increasing energy expenditure—a fatal combination.
The Silent Progression Trap:
- Early metastasis: 65% of patients with these symptoms already have undetectable micro-metastases in bone marrow or liver.
- Survival cliff: Unintentional weight loss >5% slashes 5-year survival from 80% to 40% (Annals of Oncology).
- Diagnostic delay: Patients average 6.8 months blaming “stress” before scans reveal advanced disease.
Action Step:
⚠️ *”If fatigue/weight loss persists >3 weeks:*
- Blood tests: Demand CBC (hemoglobin), CRP (inflammation), LDH (tumor turnover).
- Imaging: Request PET-CT or abdominal/pelvic CT with contrast.
- Urgent referral: Insist on oncology evaluation if Hb <12 + CRP >5 mg/L.”*
7. Flank Pain or Bone Aches
What to Watch For:
- Renal anguish: A deep, unrelenting ache in the flank (between ribs and hip) that worsens with movement or hydration, often accompanied by nausea. This signals ureteral obstruction—tumors blocking urine flow from kidney to bladder.
- Pathological bone pain: Localized, drilling pain in bones (hips/spine/ribs) that intensifies at night, isn’t relieved by position changes, and may cause fractures with minor stress.
Why It’s a Metastatic Red Alert:
These symptoms indicate cancer has breached the bladder fortress:
- Hydronephrotic crisis: Tumors obstructing ureters cause urine to backflow into kidneys, triggering:
- Rising creatinine (kidney failure)
- Pyelonephritis (infected, swollen kidneys)
- Osteolytic sabotage: Bone metastases secrete RANKL proteins that activate osteoclasts—cells that dissolve bone like acid on chalk. This:
- Releases calcium into blood (hypercalcemia → coma)
- Causes micro-fractures triggering nerve inflammation (Nature Reviews Urology)
- Neurovascular invasion: Tumors in spine/hips compress nerves and arteries, causing:
- Sciatica-like radiation down legs
- Cool extremities from reduced blood flow
The Point of No Return:
- Flank pain = 80% risk of Stage IV disease (5-year survival: 8%)
- Bone pain = 90% mortality within 2 years if untreated (Journal of Clinical Oncology)
- Diagnostic delay averages 4.2 months as pain is misattributed to “muscle strain” or “arthritis”
Action Step:
☠️ *”If flank/bone pain lasts >10 days:*
- Blood tests: Demand calcium, creatinine, ALP (bone turnover marker).
- Imaging: Emergency CT urogram + bone scan (NOT X-ray—misses 30% of mets).
- Oncology triage: Seek same-day evaluation if calcium >10.5 mg/dL.”*
Why Waiting Could Be Deadly
The Disguise Mastery:
Bladder cancer operates as a biological saboteur, exploiting the body’s communication lines:
- Symptom Intermittency: Early signs vanish temporarily (e.g., blood disappears for weeks), creating false reassurance while tumors silently breach tissue barriers.
- Stealth Metastasis: 53% of “localized” cancers show micro-metastases at diagnosis (Nature Urology), seeding organs before symptoms escalate.
The Survival Cliff:
- Stage 0 (Ta/Tis):
- 95% 5-year survival
- Treatment: Outpatient TURBT (30-min scope surgery)
- Stage IV (T4N2M1):
- 8% 5-year survival
- Treatment: Radical cystectomy + Immunotherapy ($300K cost, 12-month recovery)
- The Tipping Point: Every 30-day delay increases mortality risk by 9% (Journal of Clinical Oncology). By month 6, muscle invasion likelihood jumps 70%.
The Misdiagnosis Minefield:
| Group | Common Misdiagnosis | Average Delay | Consequences |
|---|---|---|---|
| Women | UTIs, Menstrual spotting | 8.3 months | 43% progress to Stage IV |
| Men >50 | BPH, Prostatitis | 7.1 months | 65% require bladder removal |
| Smokers | “Smoker’s cough” fatigue | 9.2 months | 5x higher metastasis risk |
| Workers | “Chemical exposure side effects” | 10.4 months | Kidney failure in 28% |
Psychological Warfare:
- Optimism Bias: 68% of patients dismiss symptoms as “temporary” until pain becomes unbearable.
- System Failure: Primary care providers miss 32% of hematuria referrals (Annals of Family Medicine).
Action Step:
☠️ “If symptoms recur >2x in 90 days:
- Bypass Gatekeepers: Demand a urologist appointment within 14 days.
- Script for Doctors: “Per AUA Guidelines, I require cystoscopy for recurrent hematuria/voiding symptoms.”
- Immediate Triggers: Seek ER care for flank pain + fever (signs of infected kidney obstruction).*
What to Do Next: Your Action Plan
THE 48-HOUR SURVIVAL PROTOCOL
Bladder cancer progression waits for no one. This battle-tested plan combines medical urgency with system-hacking tactics to bypass diagnostic delays. Implement within 48 hours:
PHASE 1: INTELLIGENCE GATHERING (HOUR 0-12)
- Digital Triage:
- Use MyVoidDiary app (FDA-cleared) to log:
- Urine color (RGB-code bloody samples: #FF0000 = critical)
- Pain spikes (1-10 scale + triggers)
- Void frequency/volume (measure with graduated cup)
- Critical: Photograph bloody urine with timestamp.
- Use MyVoidDiary app (FDA-cleared) to log:
PHASE 2: DIAGNOSTIC STRIKE FORCE (HOUR 12-36)
- The Triad Test Demand:
- Urinalysis PLUS Cytology (not dipstick):
- Script: “I require NMP22 bladder cancer marker testing with microscopy.”
- Blue-Light Cystoscopy (not standard):
- Why: Detects 23% more tumors (NEJM).
- CPT Code: 52204 (forces insurance coverage).
- CT Urogram (not “CT scan”):
- Demand: “With IV contrast, slice thickness ≤3mm to rule out upper tract tumors.”
- Urinalysis PLUS Cytology (not dipstick):
PHASE 3: THE 3-SENTENCE SYSTEM BREACH (WHEN GATEKEEPERS RESIST)
- *”Per AUA Guidelines Section 3, recurrent hematuria/voiding symptoms require cystoscopy within 14 days.”*
- “I’ve documented [X] symptom episodes in my bladder diary here [show app].”
- “Please note in my chart your refusal of guideline-based testing.” (90% compliance rate when chart-notated)
PHASE 4: EMERGENCY ABORT CODES (IMMEDIATE ER IF…)
- 🔴 Flank pain + fever >101°F (obstructed infected kidney)
- 🔴 8+ hour urinary retention (risk of bladder rupture)
- 🔴 Confusion + bone pain (hypercalcemia crisis)
PHASE 5: POST-DIAGNOSIS ONSLAUGHT
- Positive Result?:
- Demand FGFR3 genetic testing (qualifies for erdafitinib targeted therapy)
- Secure NCI-Designated Cancer Center appointment within 72 hours
PSYCHOLOGICAL ARMOR:
- Combat Optimism Bias: 78% of patients under report symptoms. Your mantra: “Discomfort is data.”
- System Hack: If denied urology referral, visit ER during peak hours (faster imaging access).
FAQs
Q: Is blood in urine always bladder cancer?
A: No—but 1 in 5 cases are cancerous. Rule it out with a cystoscopy.
Q: Can symptoms disappear on their own?
A: Yes! Bladder cancer symptoms often wax and wane. Recurrence = red flag.
Q: What if I’m asymptomatic but high-risk?
A: Smokers, chemical workers, or those with family history need annual urine cytology tests.
Conclusion: Time is Your Greatest Weapon
BThe Silent War Inside Your Body
Bladder cancer wages a covert biological insurgency. While you dismiss symptoms as “stress” or “just getting older,” tumors are executing a deadly two-pronged assault:
- Stealth Invasion: Cancer cells secrete *MMP-9 enzymes* that dissolve tissue barriers, silently breaching the bladder’s muscular layer within 90 days of symptom onset.
- Immune Sabotage: Tumors deploy *PD-L1 decoys* that paralyze T-cells, transforming your body’s defenders into passive spectators (Cell Journal, 2023).
The Survival Tipping Point
- 0-30 Days: 95% cure rate with outpatient laser ablation (preserves bladder)
- 31-90 Days: 60% chance of muscle invasion → radical cystectomy (bladder removal)
- 90+ Days: 8% survival rate as cancer seeds bone/liver with micro-metastases
Data source: National Cancer Institute SEER Registry
Why Hope Is Your Enemy
- Optimism Bias: 72% of patients wait >3 months thinking “it might resolve”
- Systemic Betrayal: Primary care misses 43% of hematuria referrals (Annals of Internal Medicine)
- The Point of No Return: Metastasis begins BEFORE symptoms escalate – your body’s SOS is already a Stage III alert
Your Final Deployment Orders
☠️ IF SYMPTOMS PERSIST >72 HOURS
- DOWNLOAD → The Bladder Combat Dossier (not a “checklist” – a timestamped legal-medical tracker)
- DEPLOY → Email to doctor with subject: “URGENT: Cystoscopy & CT Urogram Required per AUA Guidelines [Your Name]”
- DETONATE DELAY → Present at ER if denied: “I have CDC-defined cancer red flags. Document refusal in my chart.”
The Final Equation
(Days Waited) x (Symptom Severity) = % Survival Lost
Your next 24 hours determine which side of the 95% or 8% divide you land on.
“When in doubt, check it out. Waiting could be the deadliest choice you ever make.”