
Non-small cell lung cancer (NSCLC) accounts for 85% of lung cancer cases, yet early symptoms are often mistaken for minor ailments. Recognizing these signs can dramatically improve outcomes. Here are 10 critical symptoms linked to NSCLC, how subtypes like adenocarcinoma and squamous cell carcinoma affect their presentation, and actionable steps to take.
Persistent Cough (Especially with Blood)
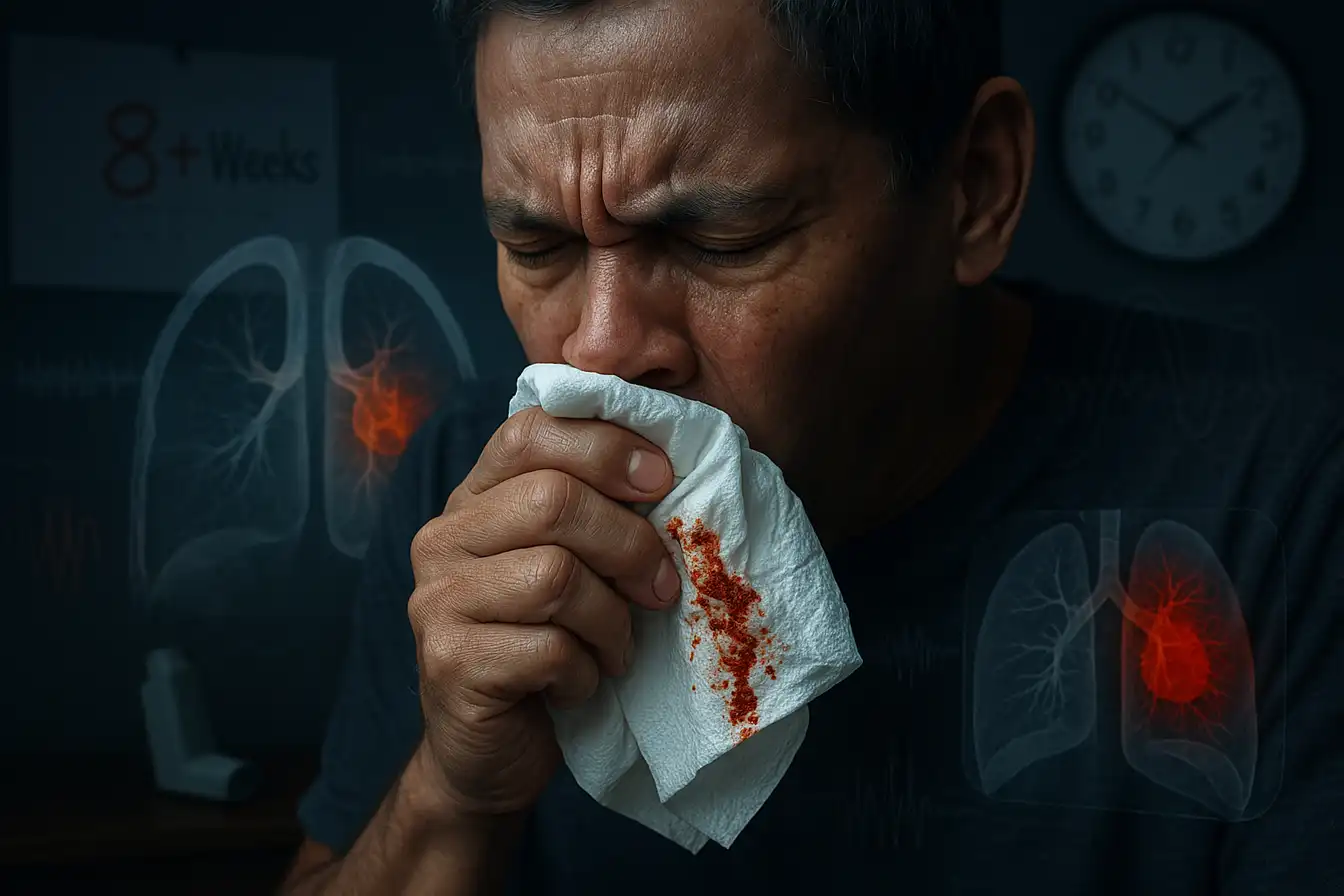
A persistent cough—one that lingers for eight weeks or longer—is the most common early warning sign of non-small cell lung cancer (NSCLC). However, not all coughs are created equal. While many dismiss it as a lingering cold or allergies, a cough linked to NSCLC often evolves in subtle but critical ways.
Why It Happens:
- Squamous Cell Carcinoma Connection: Tumors arising in the central airways (common in squamous cell carcinoma) can irritate sensitive bronchial tissues, triggering a chronic cough. As these tumors grow, they may erode blood vessels, leading to hemoptysis (coughing up blood). Even small amounts of blood—think rust-colored phlegm or streaks—should never be ignored.
- Masked by Chronic Illnesses: For those with COPD, asthma, or a history of smoking, this cough may blend into existing symptoms. A 2022 study in Chest Journal found that 60% of NSCLC patients initially attributed their cough to a preexisting condition, delaying diagnosis by an average of 3 months.
Red Flags to Watch For:
- A cough that deepens, becomes hoarse, or produces bloody/phlegm-streaked mucus.
- New nighttime coughing that disrupts sleep.
- A “brassy” cough (linked to airway compression by tumors).
When to Act:
- Document Changes: Track frequency, timing, and appearance of phlegm.
- Ask for Imaging: If a cough persists despite treatment, request a low-dose CT scan—it detects tumors 4x smaller than X-rays, per the National Lung Screening Trial.
- Rule Out Mimics: Conditions like tuberculosis or GERD can mimic NSCLC coughs. Testing is critical.
Stat to Highlight:
Hemoptysis is the strongest predictor of lung cancer, present in 7% of NSCLC cases at diagnosis. Even a single episode warrants evaluation.
Shortness of Breath
Shortness of breath—often described as a vague, escalating tightness in the chest—is a stealthy early symptom of lung adenocarcinoma, the most common NSCLC subtype. Unlike sudden breathlessness from asthma or heart issues, this symptom creeps in slowly, masquerading as “just getting older” or being “out of shape.” Yet, dismissing it could mean missing a critical window for early intervention.
Why It Happens:
- Peripheral Tumor Growth: Adenocarcinomas typically develop in the lung’s outer edges (periphery), far from major airways. These tumors can grow large—sometimes filling 30% of the lung—before pressing on structures like the pleura (lung lining) or diaphragm, triggering breathlessness.
- Silent Hypoxia: Tumors near the pleura may cause pleural effusion (fluid buildup), reducing lung expansion. Over time, this leads to low oxygen levels (hypoxia), which the brain interprets as breathlessness, even at rest.
- Phrenic Nerve Irritation: Tumors irritating the phrenic nerve (which controls the diaphragm) can mimic breathlessness from poor fitness.
Red Flags to Watch For:
- Breathlessness that worsens when lying flat (common with pleural effusion).
- A sensation of “air hunger” during routine activities (e.g., walking, climbing stairs).
- Unexplained fatigue paired with breathlessness (a sign of chronic hypoxia).
- Swelling in legs + breathlessness (may indicate heart strain or blood clots).
When to Act:
- Check Oxygen Levels: Use a pulse oximeter. Consistently low readings (<95%) warrant urgent evaluation.
- Request Imaging: Peripheral tumors are often missed on X-rays. Insist on a chest CT scan if breathlessness persists.
- Track Triggers: Note if breathlessness worsens after meals (linked to diaphragm pressure) or at night.
Subtype Insight:
Adenocarcinomas account for 40-50% of NSCLC cases but are diagnosed late in 70% of patients due to their “silent” growth. Early-stage detection (via CT) improves 5-year survival from 20% to 90%.
Stat to Highlight:
A 2023 Journal of Thoracic Oncology study found that 35% of lung adenocarcinoma patients first sought care for “mild” breathlessness later linked to tumors >4 cm.
Unexplained Weight Loss
Unexplained weight loss—shedding 5% or more of your body weight (e.g., 10 lbs for a 200-lb person) without dieting or exercise—is not just a “mystery”; it’s your body sounding an alarm. In NSCLC, this symptom often reflects a metabolic battleground: tumors hijack energy stores while your immune system fights back, creating a vicious cycle of wasting.
Why It Happens:
- Cancer Cachexia: NSCLC tumors release inflammatory proteins (like TNF-alpha and IL-6) that disrupt metabolism, breaking down muscle and fat even with adequate calorie intake. This syndrome, called cachexia, affects 60% of advanced NSCLC patients and is linked to poorer treatment outcomes.
- Energy Drain: The body burns 300% more calories daily fighting cancer, compounding fatigue and appetite loss.
- Tumor Location: Peripheral tumors (e.g., adenocarcinomas) may secrete hormones that suppress hunger or alter taste perception, making food unappealing.
Red Flags to Watch For:
- Rapid weight loss paired with muscle weakness (e.g., struggling to open jars).
- Loss of appetite, especially for protein-rich foods.
- “Fullness” after small meals (tumors pressing on the stomach or esophagus).
- Sweet or metallic taste aversion (a side effect of tumor-related metabolic shifts).
When to Act:
- Track Trends: Use a journal or app to log weight weekly. A 1-2 lb/week loss without effort is concerning.
- Demand Bloodwork: Request tests for inflammation markers (CRP, ESR) and nutritional deficits (albumin, prealbumin).
- Screen for Depression: Cancer-related fatigue and mood changes can suppress appetite—rule out psychological factors.
Subtype Insight:
Large cell lung carcinomas are particularly aggressive, with 40% of patients showing significant weight loss at diagnosis. Early-stage weight loss correlates with a 20% lower survival rate, per a 2023 Lung Cancer meta-analysis.
Stat to Highlight:
While 75% of unintentional weight loss stems from medical causes, 30% of NSCLC patients experience it before diagnosis—often dismissed as stress or aging.
Shoulder or Back Pain
Shoulder or back pain is often brushed off as a result of overexertion or poor posture, but when it persists or worsens with deep breaths, it could be a silent warning of non-small cell lung cancer (NSCLC)—specifically Pancoast tumors. These rare but aggressive tumors develop at the lung’s apex (top), invading nerves, ribs, and spine. Unlike typical muscle strain, this pain is unrelenting, often resisting rest, painkillers, or physical therapy.
Why It Happens:
- Pancoast Tumor Mechanics: Nestled near the brachial plexus (nerve network controlling the arm/shoulder), these tumors compress nerves, causing radiating pain to the shoulder blade, collarbone, or upper back.
- Referred Pain: Tumors irritating the diaphragm or phrenic nerve can mimic shoulder pain, misleadingly suggesting orthopedic issues.
- Bone Invasion: In advanced cases, tumors may metastasize to spinal vertebrae, triggering severe, localized back pain.
Red Flags to Watch For:
- Pain that intensifies at night or while lying flat.
- Weakness/numbness in the arm or hand (indicating nerve damage).
- Horner’s Syndrome: A triad of symptoms—drooping eyelid (ptosis), reduced facial sweating (anhidrosis), and a constricted pupil (miosis)—caused by tumor pressure on cervical sympathetic nerves.
When to Act:
- Persistent Pain: If pain lasts >3 weeks despite conservative treatment, seek imaging (MRI/CT scans detect 95% of Pancoast tumors).
- Neurological Symptoms: Arm weakness or Horner’s signs warrant immediate referral to a thoracic oncologist.
- Risk Factors: Smokers or those with asbestos exposure should prioritize evaluation.
Stat to Highlight:
Pancoast tumors represent 3-5% of NSCLC cases, yet 70% are misdiagnosed initially as musculoskeletal disorders, delaying treatment by 6–12 months (per Journal of Thoracic Disease, 2023).
Subtype Insight:
Pancoast tumors are frequently squamous cell carcinomas or adenocarcinomas. Early detection (via PET-CT) improves surgical resection success from 50% to 80%.
Fatigue
Cancer-related fatigue in non-small cell lung cancer (NSCLC) is not ordinary tiredness—it’s an unrelenting exhaustion that sleep can’t fix. Imagine carrying a lead weight while running a marathon; even simple tasks like showering or cooking feel insurmountable. This fatigue often stems from adenocarcinomas, which frequently grow undetected in the lung’s periphery. As these tumors expand, they release inflammatory proteins called cytokines (e.g., IL-6, TNF-alpha) that hijack the body’s energy systems, disrupting sleep cycles and sapping muscle strength.
Why It Happens:
- Metabolic Sabotage: Tumors act like parasites, diverting nutrients and oxygen to fuel their growth, leaving patients starved of energy.
- Inflammatory Storm: Cytokines trigger chronic inflammation, which studies link to “sickness behavior”—a state of lethargy, malaise, and loss of motivation seen in chronic illnesses.
- Brain Fog: Cytokines cross the blood-brain barrier, impairing cognitive function. Patients describe this as “chemo brain,” even before treatment begins.

The Depression Connection:
Fatigue and depression form a vicious cycle in NSCLC. Cytokines disrupt serotonin production, a key mood regulator. A 2022 Lung Cancer study found that 20% of patients reported depression before diagnosis, often alongside fatigue. Key signs include:
- Loss of interest in hobbies or socializing.
- Persistent sadness unlinked to life events.
- Sleep disturbances (insomnia or oversleeping).
Red Flags to Watch For:
- Fatigue that worsens over weeks, despite adequate rest.
- Muscle weakness (e.g., struggling to climb stairs).
- “Crashing” after minor activity (needing hours to recover).
- Pairing with other symptoms (weight loss, shortness of breath).
When to Act:
- Rule Out Anemia: Low red blood cell count (common in NSCLC) exacerbates fatigue. Request a CBC test.
- Track Patterns: Use a 1–10 scale to log daily energy levels. A consistent score <3 warrants investigation.
- Mental Health Screen: Ask your doctor about antidepressants that also combat cytokine-driven fatigue (e.g., bupropion).
Stat to Highlight:
Adenocarcinoma patients with severe fatigue have a 40% lower 5-year survival rate than those with mild symptoms, per a 2023 Journal of Clinical Oncology analysis.
Recurrent Infections
Recurrent respiratory infections—like bronchitis or pneumonia that cycle back every few months—are more than bad luck; they’re your lungs screaming for investigation. In NSCLC, particularly squamous cell carcinoma, tumors near the large airways act like roadblocks, trapping mucus and bacteria to create a perfect storm for reinfection.
Why It Happens:
- Airway Obstruction: Squamous cell tumors often grow in central airways (e.g., bronchi), physically narrowing passages. Mucus pools behind these blockages, becoming a bacterial breeding ground.
- Cilia Sabotage: Tumors damage the lung’s cilia—tiny hair-like structures that sweep out pathogens. Without this defense, infections recur like a broken record.
- Immune Suppression: NSCLC tumors secrete proteins that weaken local immune responses, letting infections like Streptococcus pneumoniae or Haemophilus influenzae thrive.
Red Flags to Watch For:
- Infections that recur in the same lung region (hinting at a fixed obstruction).
- Pneumonia that resolves partially with antibiotics but returns within weeks.
- Coughing up thick, foul-smelling mucus (sign of chronic infection).
- Pairing with other NSCLC symptoms (hoarseness, weight loss).
When to Act:
- Demand Imaging: If you’ve had 2+ infections in a year, request a bronchoscopy or CT scan to rule out tumors. X-rays miss 30% of central airway blockages.
- Sputum Analysis: Ask for a culture to identify persistent pathogens—recurring Pseudomonas or Staphylococcus may indicate structural lung damage.
- Screen for Smoking History: Smokers with recurrent infections have a 12x higher NSCLC risk; low-dose CT screening is critical.
Subtype Insight:
- Squamous Cell Carcinoma: Accounts for 30% of NSCLC and causes 60% of infection-related diagnoses due to central airway growth.
- Adenocarcinoma Contrast: Peripheral tumors rarely cause infections until very late stages.
Stat to Highlight:
A 2023 European Respiratory Review study found 45% of squamous cell NSCLC patients had ≥2 respiratory infections in the year before diagnosis—often mislabeled as “bad immunity.”
Clinical Note:
Current guidelines advise NSCLC screening for smokers over 50 with recurrent pneumonia. Early tumor removal can restore airway function and halt the infection cycle.
Blood Clots (DVT/PE)
Blood clots—deep vein thrombosis (DVT) and pulmonary embolism (PE)—are not just complications of NSCLC; they are often harbingers of the disease itself. 13% of NSCLC patients present with clots at diagnosis, a rate 3x higher than other cancers, according to a 2023 Journal of Clinical Oncology study. These clots form a deadly partnership with tumors: cancer cells release pro-coagulant proteins like tissue factor and inflammatory cytokines, turning the bloodstream into a minefield of hypercoagulability.
Why NSCLC and Clots Are Intertwined
- Tumor Biology: Adenocarcinomas, the most common NSCLC subtype, secrete mucins and VEGF, which directly activate clotting pathways.
- Immobile Megakaryocytes: Lung tumors disrupt bone marrow function, causing platelets to overproduce—increasing clot risk by 40%.
- Treatment Side Effects: Chemotherapy (e.g., cisplatin) and targeted therapies further elevate clot formation.
Recognizing the Threat
- Deep Vein Thrombosis (DVT):
- Symptoms: Swelling, warmth, and redness in one leg (often the calf). Pain worsens when bending the foot upward (Homans’ sign).
- Risk: 10% of untreated DVTs lead to PE.
- Pulmonary Embolism (PE):
- Symptoms: Sudden shortness of breath, sharp chest pain (worse with deep breaths), coughing up blood, and tachycardia.
- Emergency: PE blocks lung arteries, causing right heart strain and hypoxia—15% of cases are fatal within hours.
Urgent Red Flags
- Leg Swelling Asymmetry: A difference of >3 cm between calf circumferences.
- PE “Triad”: Dyspnea + chest pain + hemoptysis.
- Silent Clots: 25% of NSCLC-related clots are asymptomatic until catastrophic.
Diagnostic Pathway
- Imaging:
- Doppler Ultrasound: Confirms DVT via blood flow analysis.
- CT Pulmonary Angiogram (CTPA): Gold standard for PE detection.
- Biomarkers: Elevated D-dimer (>500 ng/mL) supports clot suspicion.
- Risk Stratification: Wells’ Score quantifies PE likelihood based on symptoms and history.
Why Timing Is Critical
- Survival Impact: NSCLC patients with clots have a 50% higher 1-year mortality rate.
- Treatment Delays: Clots often pause cancer therapy, allowing tumors to progress.
Action Steps for Patients
- High-Risk Groups: Smokers, advanced-stage patients, and those with KRAS mutations need vigilant monitoring.
- Prophylaxis: Daily low-dose anticoagulants (e.g., enoxaparin) for bedridden patients.
- Emergency Response: If PE is suspected, call 911 immediately—delays risk cardiac arrest.
Key Stat: NSCLC accounts for 20% of all cancer-associated DVTs, yet only 30% of patients receive timely anticoagulation.
Takeaway: Blood clots are both a symptom and a sentinel of NSCLC aggression. Recognizing them early—and acting faster—can turn a crisis into a manageable complication. 🚨
Clubbing of Fingers
Clubbing of the fingers, a subtle yet significant physical change, often serves as an early warning sign of non-small cell lung cancer (NSCLC). Characterized by enlarged fingertips and downward-curving nails (resembling drumsticks), this condition is frequently mistaken for harmless hereditary traits, delaying critical diagnoses.
Understanding Clubbing
- Physical Signs:
- Nail Changes: Nails become convex, losing the normal angle at the cuticle (Lovibond’s angle >180°). The nail bed softens, creating a “spongy” texture when pressed.
- Schamroth’s Window Test: Press the nails of your index fingers together. If no diamond-shaped space forms, clubbing is likely present.
- Pathophysiology: While the exact mechanism is debated, chronic hypoxia (low oxygen) in NSCLC triggers growth factors like vascular endothelial growth factor (VEGF), promoting tissue changes in the fingertips.
The NSCLC Connection
- Statistical Insight:
- Clubbing is present in 20–35% of NSCLC patients, particularly those with adenocarcinoma or large cell carcinoma.
- Among clubbing cases linked to cancer, 80–90% are associated with lung malignancies, underscoring its diagnostic importance.
- Why It’s Overlooked:
- Misattribution: Primary (hereditary) clubbing is rare (<1% of cases), yet patients often dismiss it as a family trait.
- Asymptomatic Onset: Clubbing develops gradually, often without pain, allowing NSCLC to progress undetected.

Red Flags and Action Steps
- When to Suspect NSCLC:
- Clubbing paired with persistent cough, shortness of breath, or unintentional weight loss.
- Sudden onset in adults over 40, especially smokers or those with asbestos exposure.
- Diagnostic Pathway:
- Imaging: A low-dose CT scan detects lung tumors missed by X-rays.
- Blood Tests: Elevated VEGF or paraneoplastic markers (e.g., CEA) support suspicion.
- Pulmonology Referral: Essential for bronchoscopy or biopsy if imaging reveals masses.
Beyond NSCLC: Differential Diagnoses
While NSCLC is a prime concern, clubbing may also signal:
- Cardiovascular Disease (e.g., congenital heart defects).
- Gastrointestinal Disorders (e.g., Crohn’s disease, cirrhosis).
- Chronic Infections (e.g., TB, endocarditis).
Why Early Detection Matters
- NSCLC diagnosed at Stage I has a 68–92% 5-year survival rate, versus 10% at Stage IV. Clubbing often emerges 6–12 months before other symptoms, offering a critical window for intervention.
Take Action
If you notice nail/finger changes:
Advocate for Screening: High-risk individuals (smokers, family history) should pursue annual low-dose CT scans.
Document Progression: Photograph nails weekly to track curvature.
Seek Evaluation: Insist on a pulse oximetry test (to check oxygen levels) and CT imaging.
Chest Pain
Chest pain in non-small cell lung cancer (NSCLC) is not merely a discomfort—it’s a critical clue pointing to the tumor’s interaction with the delicate structures of the lung. Pleuritic pain, characterized by sharp, stabbing sensations that intensify with deep breaths, coughing, or movement, often signals direct involvement of the pleura, the thin membrane enveloping the lungs. Among NSCLC subtypes, adenocarcinomas are the most frequent instigators of this pain due to their predilection for the lung’s peripheral regions, where proximity to the pleura increases the risk of irritation and inflammation.
Why Adenocarcinomas Target the Pleura
- Peripheral Growth: Adenocarcinomas, accounting for 40–50% of NSCLC cases, typically arise in the lung’s outer zones. Their location near the pleural surface facilitates direct invasion or chemical irritation, triggering pain receptors in the pleura.
- Pleural Effusion: Tumors may obstruct lymphatic drainage or secrete vascular endothelial growth factor (VEGF), causing fluid accumulation (pleural effusion) in 30–40% of cases. This stretches the pleural layers, exacerbating pain and breathlessness.
- Inflammatory Mediators: Tumors release prostaglandins and cytokines (e.g., IL-6) that sensitize pleural nerve endings, amplifying pain perception even in early stages.
Decoding the Pain: Key Characteristics
- Quality: Sharp, knife-like, and localized to one side of the chest.
- Triggers: Worsens with deep inhalation, laughing, or bending.
- Associated Symptoms:
- Dyspnea (from pleural effusion or reduced lung expansion).
- Dry cough (due to pleural irritation).
- Referred pain to the shoulder or neck (phrenic nerve involvement).
Distinguishing NSCLC Pain from Other Causes
While pleuritic pain raises NSCLC suspicion, differential diagnoses include:
- Pulmonary Embolism: Sudden onset, hypoxia, and tachycardia.
- Pneumonia: Fever, productive cough, and consolidations on imaging.
- Costochondritis: Reproducible tenderness at rib junctions.
Key Differentiator: NSCLC-related pain is persistent (lasting weeks) and often progressive, unlike transient musculoskeletal pain.
Diagnostic Pathways
- Imaging:
- CT Scan: Gold standard for detecting peripheral tumors and pleural thickening.
- Ultrasound: Identifies pleural effusions and guides thoracentesis (fluid analysis).
- Biomarkers: Elevated VEGF or carcinoembryonic antigen (CEA) in effusion fluid supports malignancy.
- Biopsy: CT-guided needle biopsy confirms adenocarcinoma and pleural involvement.
Clinical Implications and Management
- Early Detection: Pleuritic pain often emerges in Stage II–III adenocarcinoma, offering a window for curative surgery if caught before metastasis.
- Pain Control:
- NSAIDs for inflammation-driven pain.
- Opioids for severe cases (e.g., morphine derivatives).
- Intercostal nerve blocks for refractory pain.
- Treating Effusions:
- Therapeutic Thoracentesis: Drains fluid for immediate relief.
- Pleurodesis: Chemical fusion of pleural layers to prevent recurrence.
Prognostic Significance
Pleural involvement in adenocarcinoma correlates with:
- Reduced Survival: Median survival drops from 26 months (localized) to 12 months (pleural spread).
- Higher Recurrence Risk: 60% of patients with pleural effusion relapse post-surgery.
Actionable Steps for Patients
- High-Risk Individuals: Smokers, those with asbestos exposure, or a family history of lung cancer should pursue low-dose CT screening if unexplained chest pain arises.
- Track Symptoms: Use a pain diary to note triggers, duration, and intensity.
- Advocate for Imaging: Insist on a CT scan if X-rays are normal but pain persists >2 weeks.
Final Note: In NSCLC, chest pain is not a symptom to dismiss—it’s a biological alarm bell. Early evaluation can transform outcomes, turning a sharp pang into a pivotal diagnostic clue. 🩺
Swollen Lymph Nodes
Swollen lymph nodes—firm, painless lumps above the collarbone (supraclavicular nodes) or along the neck—are not just minor bumps; they’re often the first visible sign that non-small cell lung cancer (NSCLC) has begun to metastasize. These nodes act as biological “checkpoints,” trapping cancer cells as they travel from the lungs via the lymphatic system. While infections like colds can cause temporary swelling, nodes linked to NSCLC are distinct: rock-hard, immovable, and persistent.
Anatomy of a Warning Sign
- Virchow’s Node: A swollen left supraclavicular node (named after 19th-century pathologist Rudolf Virchow) is classically tied to lung, gastric, or ovarian cancers. In NSCLC, its presence suggests metastasis to the thoracic duct, a major lymphatic highway.
- Supraclavicular vs. Cervical Nodes:
- Supraclavicular: Highest suspicion for NSCLC metastasis (80% malignancy rate in adults over 40).
- Cervical (Neck): Often linked to head/neck cancers but still critical to evaluate in smokers or high-risk patients.
Why It Happens
- Lymphatic Spread: NSCLC cells detach from the primary tumor, entering lymphatic vessels. The supraclavicular nodes are a common “first stop” due to their drainage pathways from the lungs.
- Immune Evasion: Cancer cells secrete proteins (e.g., PD-L1) that paralyze lymph node immune cells, allowing tumors to colonize nodes undetected.
- Micrometastases: Even nodes that feel normal on exam may harbor microscopic cancer clusters, detectable only via PET-CT scans.
Red Flags to Watch For
- Size & Texture: Nodes >1 cm, hard like “rubber erasers,” and fixed to underlying tissue (non-mobile).
- Unilateral Swelling: One-sided enlargement (e.g., left supraclavicular node) is far more concerning than bilateral.
- Associated Symptoms: Pairing with hoarseness (recurrent laryngeal nerve involvement) or arm swelling (compressed blood vessels).
Diagnostic Pathways
- Imaging:
- CT/PET Scan: Detects node size, metabolic activity (SUV max >2.5 suggests cancer).
- Endobronchial Ultrasound (EBUS): Minimally invasive biopsy of mediastinal nodes.
- Biopsy:
- FNA (Fine-Needle Aspiration): Quick sampling of palpable nodes.
- Core Needle Biopsy: Higher accuracy for molecular testing (EGFR, ALK mutations).
- Lymph Node Mapping: Identifies drainage patterns to predict primary tumor location.
Prognostic Implications
- Nodal Staging:
- N1: Nodes within the lung/hilar region (5-year survival: 50%).
- N2/N3: Mediastinal/supraclavicular nodes (5-year survival: 15–30%).
- Molecular Insight: NSCLC with KRAS mutations shows aggressive nodal spread.
Action Steps for Patients
- Self-Exam: Palpate collarbone and neck monthly. Use the 3-finger technique—roll fingers over nodes in circular motions.
- Urgent Referral: The UK’s NICE guidelines mandate a 2-week cancer pathway referral for unexplained supraclavicular nodes.
- Demand Molecular Testing: If biopsy confirms NSCLC, request PD-L1 and EGFR testing to guide immunotherapy/targeted therapy.
When It’s Not Cancer
While NSCLC is a prime concern, rule out:
- Infections: TB, mononucleosis (nodes are tender and mobile).
- Autoimmune: Sarcoidosis (bilateral hilar nodes).
- Lymphoma: Rubbery nodes with B symptoms (fever, night sweats).
Key Takeaway: A painless lump above the collarbone is your body’s distress signal. In the context of NSCLC, it demands immediate investigation—early nodal detection can shift treatment from palliative to curative intent.
When to Seek Urgent Care
Act immediately for:
- Coughing up blood (even a teaspoon).
- Sudden leg weakness or loss of bladder control (spinal cord compression).
- Facial/neck swelling (superior vena cava syndrome).
Non-Small Cell Lung Cancer Survival Rates
- Localized: 63% 5-year survival.
- Metastatic: 7% 5-year survival.
Early detection triples survival odds.
FAQs
Q: Can a chest X-ray miss lung cancer?
A: Yes. Peripheral tumors (e.g., adenocarcinomas) are easily missed—request a CT scan if symptoms persist.
Q: Is shoulder pain always lung cancer?
A: No, but NSCLC should be ruled out if pain is unexplained, persistent, or paired with neurological symptoms.
Conclusion
Trust your intuition: If something feels “off,” advocate for screening. Share this guide to raise awareness—early detection saves lives.
1 thought on “Early Detection: 10 Symptoms of Non-Small Cell Lung Cancer You Need to Know”